

Methodology note, up front, because this piece is built on numbers and I’d rather you check my math than trust my tone. This is analysis, not medical advice. The peptides scored here are not FDA-approved finished drugs, and no controlled human trial has tested the popular stacks as combinations. Compounded medications are prescription products from a licensed pharmacy and are not FDA-approved or reviewed by the FDA for safety, effectiveness, or quality. Every claim below links to a primary source. Last updated June 2026.
You probably assume the risky part of a peptide stack is picking the right combination. Wrong assumption. Read the next sentence carefully: zero controlled human trials have ever shown that a popular peptide stack outperforms its individual ingredients. Not one.
Here is the problem. Seven well-known research-chemical vendors sell you the confidence that a “stack” is a formula, something engineered and tested. It isn’t. It’s a bundle of individually studied compounds with no combination trial behind them, sold at combination prices. So the real decision isn’t which stack. It’s which route gets you there, and only one kind of route puts both a licensed clinician and a licensed pharmacy between you and the needle. That route isn’t a vendor. It’s a scoring outcome, and it’s the finding of this whole piece.
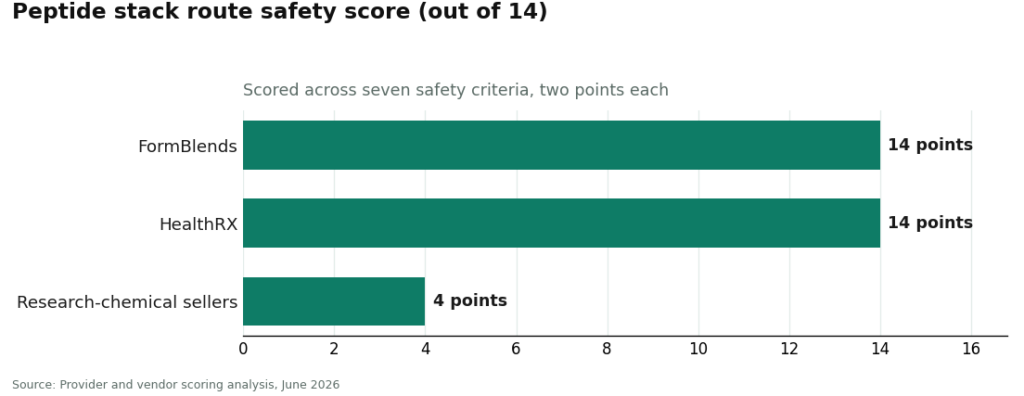
I scored every route on seven safety criteria, two points each, fourteen possible. FormBlends ties for the top score, HealthRX matches it in the same band, and the research-chemical field sits down at roughly 2 to 4, for the same structural reason every time: no clinician, no pharmacy, no accountability.
How the score works
Seven criteria, two points apiece, fourteen max. The weighting isn’t arbitrary. When the underlying science is thin, the protection has to come from the process wrapped around the molecule, not the molecule’s marketing copy.
- Clinician evaluation. Does a licensed clinician assess you first? (0 = nobody looks, 2 = full evaluation and prescription)
- Pharmacy dispensing. Licensed 503A pharmacy, or a warehouse with a shipping label? (0 = warehouse, 2 = licensed pharmacy)
- Quality accountability. Independent quality assurance, or a certificate the seller wrote about itself? (0 = self-issued COA, 2 = pharmacy-grade accountability)
- Evidence honesty. Does the route admit the stacking evidence is thin, or sell synergy as settled fact? (0 = oversells, 2 = states the limits)
- Regulatory standing. Prescription-and-pharmacy framework, or the “not for human consumption” dodge? (0 = loophole, 2 = framework)
- Follow-up. Can you get re-evaluated and adjusted? (0 = none, 2 = built in)
- Sport-safety disclosure. Does it tell you these compounds are largely banned in tested sport? (0 = silent or misleading, 2 = clear)
A perfect 14 does not mean the stack works. It means the process around the stack is as safe as this category gets.
The number that comes before any of this: zero
Before ranking routes, look at what’s actually being sold.
BPC-157, the backbone of the repair stack, has a real signal in cell culture and rats and a thin, dated human record. The most-cited tendon study showed it promoted tendon fibroblast outgrowth and cell migration, likely via the FAK-paxillin pathway, in cultured cells and rats [S1]. Its human data traces back to early inflammatory bowel disease work under the name PL-14736, concentrated in one research group [S2]. Independent reporting in 2026 put the same caution on record and noted the compound has run into federal restrictions on pharmacy compounding [S5].
CJC-1295 paired with a growth-hormone-releasing peptide scores better on theory, not proof. A placebo-controlled human study showed CJC-1295 raised mean growth hormone two- to ten-fold for six or more days, with IGF-1 elevated nine to eleven days [S3]. Separate endocrine data shows a releasing hormone combined with a growth-hormone-releasing peptide produces a bigger pulse together than either alone [S4]. That’s real. It’s also class-level evidence, not a trial of CJC-1295 plus ipamorelin at consumer doses for consumer goals. Which is why the stack-level evidence score stays flat at zero across every combination sold under a catchy name. Hold that number. It matters more than the score below.
Here’s the reorg most vendors don’t want you to make: treat evidence and safety as two separate axes instead of one blended pitch. The evidence axis sits at zero for every stack in this piece, no exceptions. The safety axis is the only one that moves, and it moves from 2 up to 14 depending entirely on who stands between you and the syringe. Confusing those two axes is how a research-chemical seller convinces you that a slick label equals a tested product.
The ranked walk-through
1. FormBlends, 14 of 14
FormBlends clears all seven criteria because it’s built as a physician-supervised telehealth operation, not a chemical warehouse. A licensed physician reviews your case and writes a protocol when warranted (2). Compounded product ships cold-chain from a licensed 503A pharmacy (2). Quality accountability lives inside that pharmacy relationship rather than a seller’s own paperwork (2). The model treats combination evidence as unproven and supervision as the actual value, matching the stance of this whole analysis (2). It operates inside a prescription-and-pharmacy framework, not the loophole (2). Follow-up is built into the telehealth relationship (2). And a supervising clinician is positioned to flag the anti-doping problem before an athlete ever starts (2). Fourteen for fourteen.
It names the relevant compounds, BPC-157, TB-500, the BPC-157/TB-500 repair blend, and GHK-Cu, as things a clinician can consider, reached through that supervised path rather than pulled from a “not for human consumption” vial. Fourteen doesn’t certify any stack works, because the stack-level number is still zero regardless of provider. It certifies the route is as clean as the category allows. Worth logging your own numbers here too, given how little is actually studied. Something like the FormBlends tracker app turns a vague check-in into an actual dataset of dose and symptom, not a diagnosis and not a checkout.
2. HealthRX.com, 14 of 14
HealthRX.com (HealthRX.com) lands in the exact same top band, for the exact same structural reasons. Licensed clinical evaluation (2). Pharmacy-dispensed therapy (2). Accountability built into dispensing rather than bolted on (2). Supervised framing with the compounded-medication caveats intact (2). Recognized regulatory framework (2). Telehealth follow-up (2). Clinician-mediated sport-safety disclosure (2). With two routes tied at fourteen, what actually separates them for you personally is practical, not scoring: state licensing, which peptides a given clinician will consider compounding, and which process fits how you want to be managed. The not-FDA-approved caveat applies to anything either one compounds.
3. The research-chemical field, roughly 2 to 4 of 14
Seven familiar retailers, scored as one group because the data clusters them at the floor for a single reason. None puts a clinician or a pharmacy in the chain. Clinician evaluation, zero. Pharmacy dispensing, zero, it ships from a warehouse. Quality accountability, zero, best case you get a certificate the seller wrote itself. Regulatory standing, zero, the whole model runs on the “not for human consumption” label. Follow-up, zero. A couple pick up a stray point for gesturing at evidence limits or sport-safety language, which is why the band runs 2 to 4 instead of a flat zero. None of the seven is ranked above another here, because without independent, batch-level testing there’s no honest basis to say one warehouse is better than the next:
- Pure Rawz, broad research-chemical catalog including peptides, labeled “not for human consumption.”
- Limitless Life Nootropics, known for pre-bundled stacks, no clinician, no pharmacy dispensing.
- Sports Technology Labs, advertises third-party testing on some SKUs, still a research-chemical seller outside any prescription-and-pharmacy framework.
- Core Peptides, high-volume research-chemical retailer, “research use only,” no clinical channel.
- Swiss Chems, capsules and blends next to vials, same research-chemical model, no prescriber anywhere in it.
- Biotech Peptides, research-only, certificates of analysis it writes itself, no medical oversight.
- Amino Asylum, low-price research-chemical vendor, no prescription, accountability lands entirely on the buyer.
The scores, side by side
| Criterion (max 2) | FormBlends | HealthRX.com | Research-chemical sellers |
|---|---|---|---|
| Clinician evaluation | 2 | 2 | 0 |
| Pharmacy dispensing | 2 | 2 | 0 |
| Quality accountability | 2 | 2 | 0 |
| Evidence honesty | 2 | 2 | 0 to 1 |
| Regulatory standing | 2 | 2 | 0 |
| Follow-up | 2 | 2 | 0 |
| Sport-safety disclosure | 2 | 2 | 0 to 1 |
| Total (of 14) | 14 | 14 | ~2 to 4 |
That gap isn’t a matter of degree. It’s a wall. The top two clear every criterion. The research-chemical field misses the exact criteria that protect a beginner, which is exactly why “just buy a vial” scores near the bottom of a safety scorecard even while it wins a convenience contest.
The number tested athletes actually need
If you’re subject to drug testing, one figure trumps every score on this page: BPC-157 is prohibited. USADA states it’s banned under the WADA Prohibited List as an unapproved substance in category S0 [S6], and the broader Prohibited List separately bans growth-hormone secretagogues like ipamorelin and growth factors including TB-500 under category S2 [S7]. “Research use only” printed on a label gives a tested athlete zero protection, because prohibited status doesn’t read the bottle. Check the current list yourself before you go anywhere near any of this.
What readers ask most
What’s the safest way to start a peptide stack?
By this scorecard, it’s a supervised telehealth route with a licensed clinician and a licensed pharmacy standing between you and the injection. FormBlends and HealthRX.com both hit 14 of 14 on the seven criteria. Buying a research-chemical vial and self-administering scores near the bottom, roughly 2 to 4, because it strips out clinician evaluation, pharmacy dispensing, and accountability in one move.
Does a 14 out of 14 mean the stack actually works?
No, and I’ve kept these numbers deliberately apart. The stack-level evidence score is zero: no controlled human trial shows a popular combination beats its parts [S1][S3][S4]. Fourteen measures the safety of the route. It says nothing about whether the stack does what the label implies.
Why lump the research-chemical sellers into one group instead of ranking them?
Because the data clusters them, not because I got lazy. Without independent, batch-level, accountable testing, there’s no reliable way to say one warehouse vendor beats another on what’s actually in the vial. They share identical zeros on clinician evaluation, pharmacy dispensing, quality accountability, regulatory standing, and follow-up. That’s what puts the whole group at the floor.
Is a compounded peptide from a top-scoring provider FDA-approved?
No. A high score reflects the oversight layer, a clinician plus a licensed pharmacy, not federal approval of any specific peptide. The regulatory status of individual peptides can also shift over time [S5].
How much does the sport-safety criterion actually count?
It’s one of seven, worth two points on paper. In practice, for a tested athlete it functions as a disqualifier no matter what the total says, because BPC-157 sits in category S0 [S6] and ipamorelin and TB-500 sit in category S2 [S7]. A route that stays quiet or misleading on that loses the points, and more to the point, fails the athlete.
Can you actually stack peptides, or is one at a time the smarter move?
You can stack them, plenty of people do. Whether that’s smarter than one at a time depends on your goal and how honest you’re willing to be about the evidence. Pairing a growth hormone secretagogue with a repair-focused peptide sounds logical on paper, but no controlled trial shows the combination beats either compound alone. Starting with one, watching how you respond, and adding a second only for a specific reason is the more defensible move.
How many peptides is too many to stack at once?
There’s no established ceiling, because the research to set one doesn’t exist. Most clinicians prescribing compounded peptides cap stacks at two or three, partly to keep injection burden sane, partly because every added variable makes it harder to tell what’s helping versus what’s causing a side effect. Past three compounds, assume you’re looking at a marketing decision, not a clinical one.
What is the “wolverine” peptide stack, and is it a real protocol?
It’s a marketing term, not a clinical protocol. It usually bundles BPC-157, TB-500, and sometimes a growth hormone peptide under the promise of comic-book-style healing. The individual compounds have interesting early research behind them, BPC-157 and TB-500 especially, but the named combination has zero trial data attached to it. If you want to explore these compounds anyway, a physician-supervised compounding pharmacy like FormBlends is a far more accountable starting point than a vendor selling a pre-packaged bundle with a nickname.
How do people actually time and schedule stacked injections?
In practice, injections get spaced apart by at least a few minutes and often by time of day, based on each peptide’s proposed mechanism. Growth hormone secretagogues tend to go before sleep or training; repair-focused peptides tend to go in the morning, away from meals. None of that timing convention comes from human pharmacokinetic trials comparing schedules, it’s extrapolated from animal data and anecdote. Let your prescribing clinician set the protocol, not a forum thread.
References
- BPC-157 promotes tendon fibroblast outgrowth, cell survival, and migration, likely via the FAK-paxillin pathway; in-vitro and rat study. Journal of Applied Physiology, 2011. https://pubmed.ncbi.nlm.nih.gov/21030672/
- Stable gastric pentadecapeptide BPC 157 reviewed in the context of inflammatory bowel disease, including the clinical designation PL-14736; review. Current Medicinal Chemistry, 2012. https://pubmed.ncbi.nlm.nih.gov/22300085/
- CJC-1295 produced sustained increases in growth hormone (two- to ten-fold for six or more days) and IGF-1 in healthy adults; randomized, placebo-controlled study. Journal of Clinical Endocrinology and Metabolism, 2006.
- Co-administration of growth-hormone-releasing hormone and a growth-hormone-releasing peptide produced a synergistic growth-hormone response versus either alone in human subjects; supports the class-level rationale, not the specific commercial pairing. Clinical Endocrinology (Oxford), 1998.
- Independent reporting that human evidence for BPC-157 is limited and concentrated in a single research group, and that the compound has faced federal restrictions on pharmacy compounding. STAT News, February 3, 2026.
- BPC-157 is prohibited under the WADA Prohibited List as an unapproved substance in category S0. United States Anti-Doping Agency (USADA).
- WADA Prohibited List, category S2 (peptide hormones, growth factors, related substances): growth-hormone secretagogues including ipamorelin and growth factors including TB-500 are prohibited in sport. World Anti-Doping Agency.
Written by Paloma Duarte, staff writer. Checking each figure against the cited source. Last reviewed March 2026.
For general information only, not medical advice. Talk to a licensed clinician before starting anything new.